Irritable Bowel Syndrome (IBS): When the Gut Speaks Without Disease
Introduction
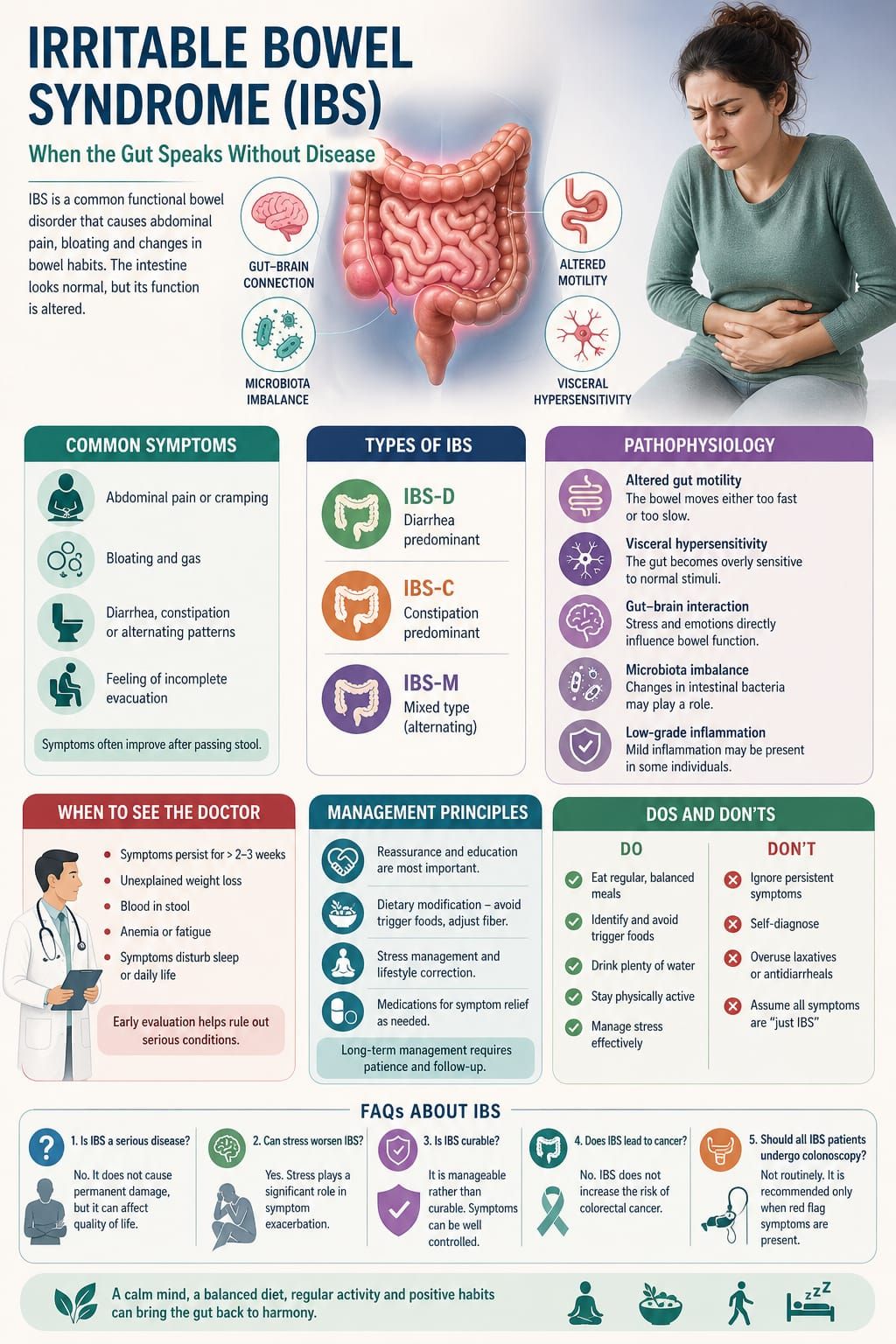
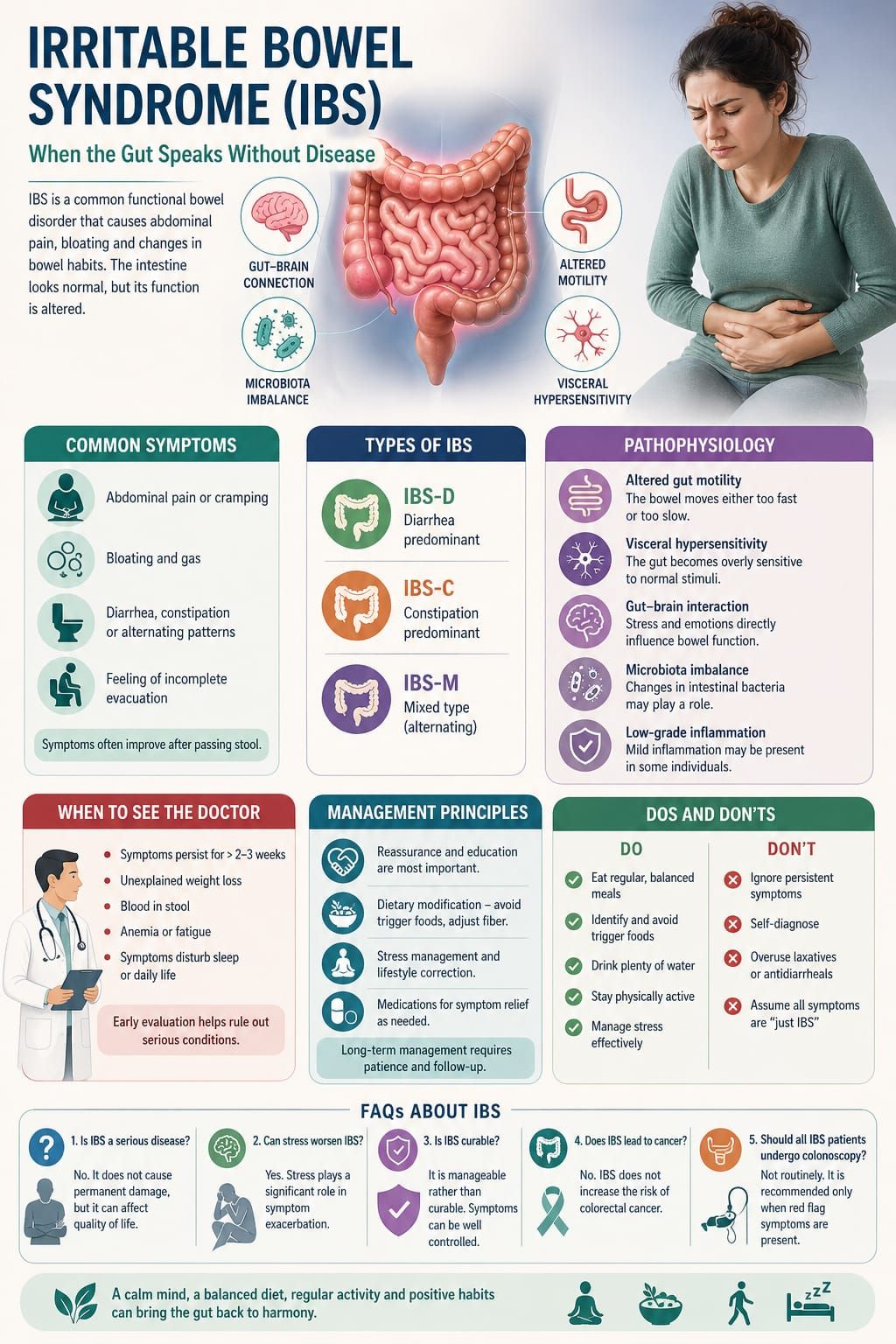
In clinical practice, few conditions challenge both the physician and the patient as much as Irritable Bowel Syndrome (IBS). It presents with real, often distressing symptoms, yet routine investigations frequently return normal results. This paradox—significant discomfort without identifiable structural disease—makes IBS a unique and often misunderstood condition.
IBS is not a disease of damage; it is a disorder of function. The gut appears normal, yet behaves abnormally. Understanding this distinction is essential for both effective management and patient reassurance.
General Readers
Many individuals experience digestive discomfort at some point—bloating, abdominal pain, irregular bowel habits. In IBS, these symptoms become recurrent and persistent.
Patients commonly report:
• Abdominal pain or cramping
• Bloating and gas
• Diarrhea, constipation, or alternating patterns
• A sense of incomplete bowel evacuation
A key feature is that symptoms often improve after passing stool.
Importantly, IBS does not lead to serious complications like cancer or permanent intestinal damage. However, it can significantly affect daily life, mood, and social functioning.
Medical Students
IBS is classified as a functional gastrointestinal disorder.
Diagnostic Considerations
• Based primarily on clinical criteria (e.g., symptom patterns)
• Absence of structural or biochemical abnormalities
• Diagnosis of exclusion only when red flags are present.
Subtypes
• IBS-D (diarrhea predominant)
• IBS-C (constipation predominant)
• IBS-M (mixed type)
Key Clinical Insight
The diagnosis relies more on pattern recognition than on investigations. Over-testing should be avoided in typical cases.
Young Doctors
IBS requires a careful balance between clinical confidence and diagnostic caution.
Important clinical points:
• Do not dismiss symptoms as “psychological”
• At the same time, avoid unnecessary extensive investigations
• Look actively for red flags:
• Weight loss
• Blood in stool
• Anemia
• Nocturnal symptoms
The doctor’s explanation plays a therapeutic role. A clear, confident diagnosis often reduces patient anxiety and improves outcomes.
General Practitioners
IBS is extremely common in primary care settings.
Practical Clinical Approach
• Take a detailed history:
• Relation of pain with bowel habits
• Dietary triggers
• Stress factors
• Minimal essential investigations:
• CBC
• Basic stool examination (if indicated)
Management Principles
• Reassurance is key
• Dietary advice (fiber adjustment depending on subtype)
• Address stress and lifestyle factors
• Symptomatic treatment:
• Antispasmodics
• Laxatives or antidiarrheal agents as needed
Long-term doctor-patient relationship plays a crucial role in management.
Pathophysiology
IBS is best understood as a disorder of the gut-brain axis.
Several mechanisms contribute:
• Altered gut motility
Either increased or decreased intestinal movement
• Visceral hypersensitivity
The gut becomes overly sensitive to normal stimuli
• Gut-brain interaction
Emotional stress directly influences bowel function
• Microbiota imbalance
Changes in intestinal flora may play a role
• Low-grade inflammation (in some cases)
These factors interact in a complex manner, explaining the variability of symptoms among patients.
When to See the Doctor
Medical consultation is necessary if:
• Symptoms persist for several weeks
• There is unexplained weight loss
• Blood appears in stool
• There is anemia or fatigue
• Symptoms disturb sleep
Early evaluation helps differentiate IBS from more serious conditions.
Irritable Bowel Syndrome is not a disease of visible damage, but a disorder of function and regulation. It reflects the deep connection between the gut and the mind, where physical symptoms often mirror internal stress and imbalance.
For the physician, IBS requires patience, understanding, and clear communication. For the patient, it requires awareness, lifestyle adjustment, and trust in the management process.
In IBS, healing does not come from a single medication—it comes from restoring balance within the body.
Dos and Don’ts
Do
• Maintain regular meal timings
• Identify and avoid trigger foods
• Stay physically active
• Manage stress effectively
Don’t
• Ignore persistent symptoms
• Self-diagnose without medical advice
• Overuse laxatives or antidiarrheal drugs
• Assume all symptoms are “just IBS” without evaluation
FAQs About Irritable Bowel Syndrome (IBS)
1. Is IBS a serious disease?
No. It does not cause permanent damage, but it can affect quality of life.
2. Can stress worsen IBS?
Yes. Stress plays a significant role in symptom exacerbation.
3. Is IBS curable?
It is manageable rather than curable. Symptoms can be well controlled.
4. Does IBS lead to cancer?
No. IBS does not increase the risk of colorectal cancer.
5. Should all IBS patients undergo colonoscopy?
Not routinely. It is recommended only when red flag symptoms are present.

By Dr. Mohammed Tanweer Khan
A Proactive/Holistic Physician
Founder of WithinTheBody.com