Gastroesophageal Reflux Disease (GERD): When Acid Becomes a Problem
Introduction
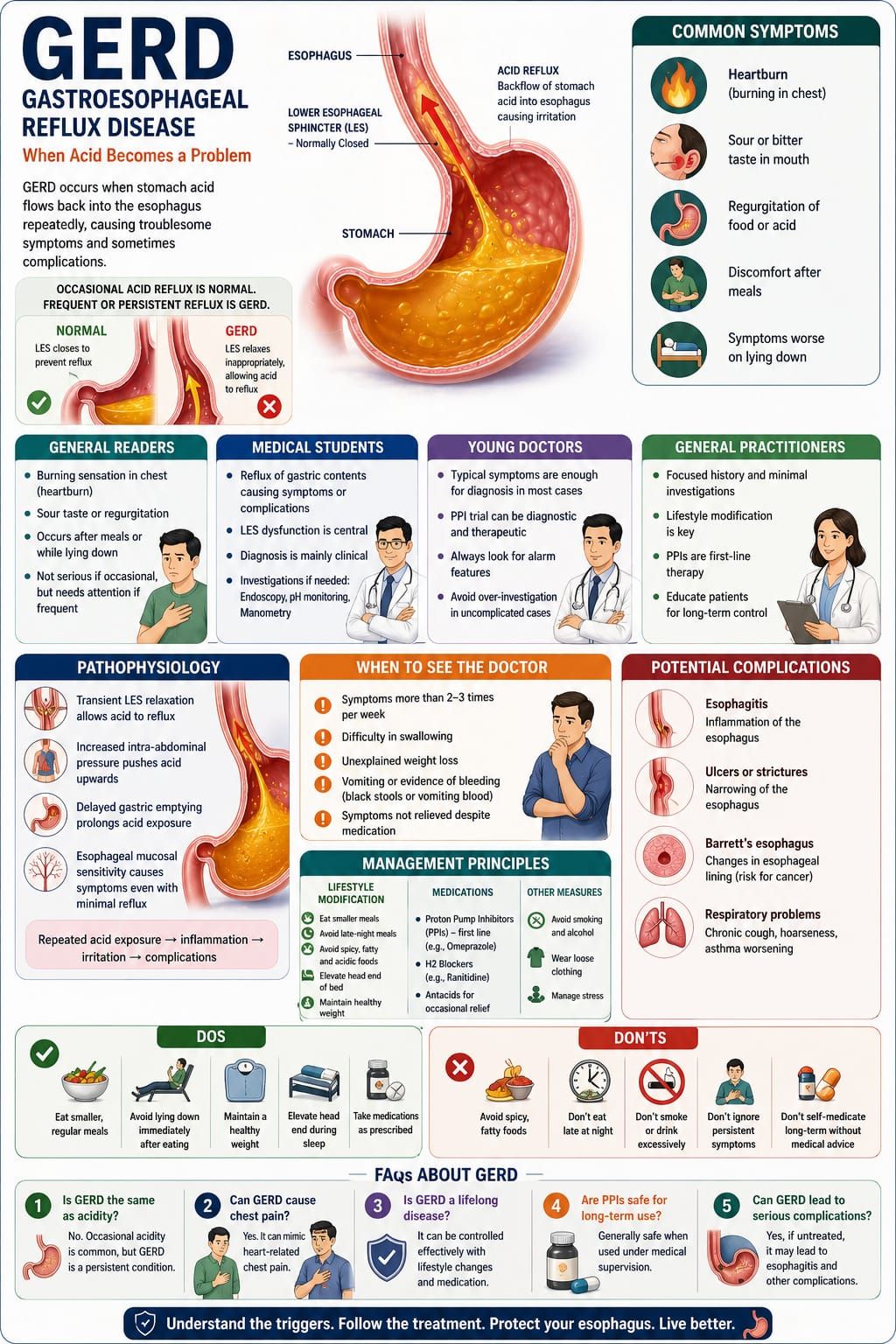
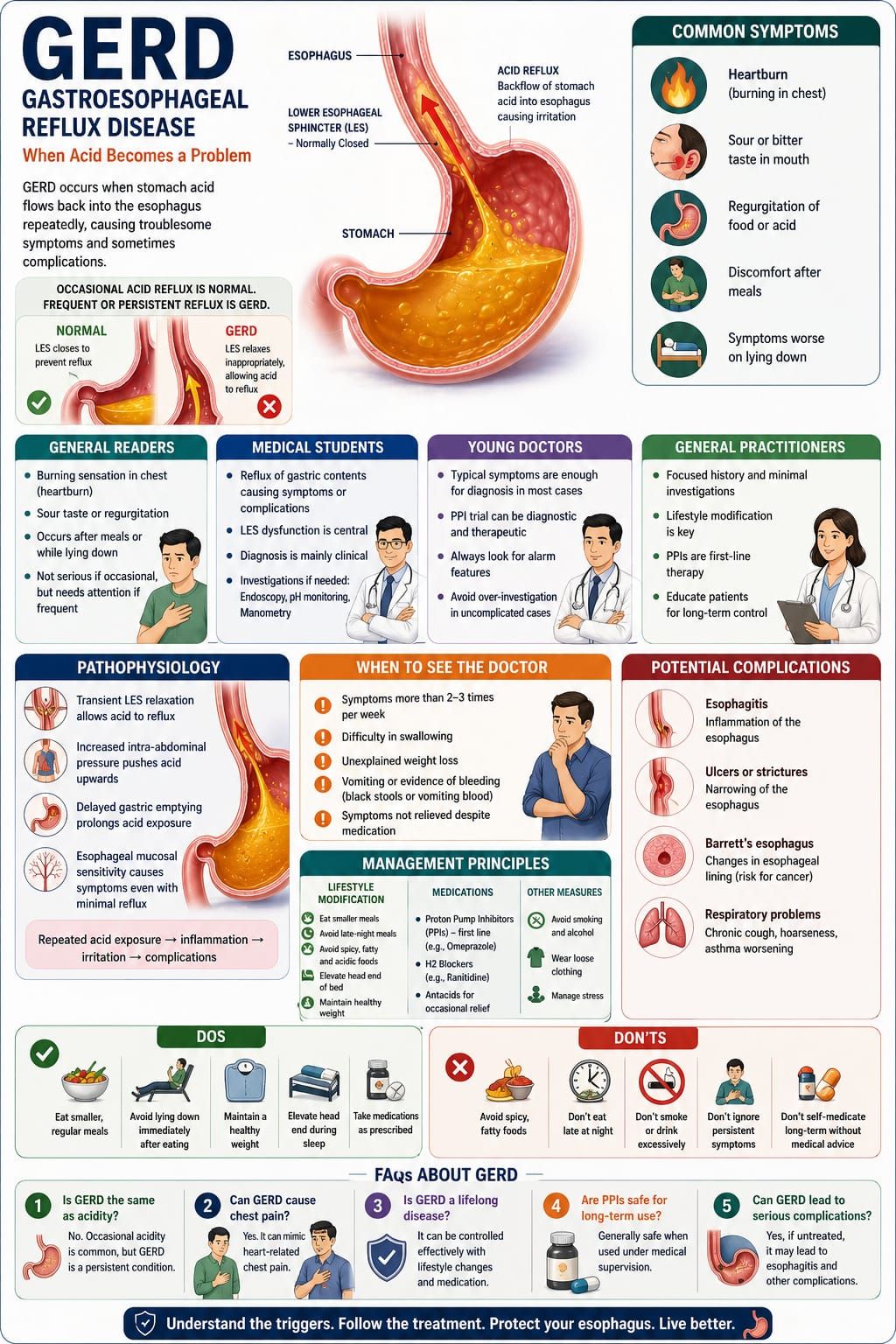
Gastroesophageal Reflux Disease (GERD) is one of the most frequently encountered conditions in clinical practice. It represents a disturbance not of structure, but of function—where the normal barrier between the stomach and the esophagus fails to maintain its integrity.
Occasional acid reflux is common and often harmless. However, when this reflux becomes frequent and persistent, it evolves into a disease state, leading to symptoms and potential complications.
GERD is not merely about acidity—it is about the inappropriate movement of gastric contents into a region not designed to tolerate them.
General Readers
Many people are familiar with the sensation of “acidity” or heartburn—a burning feeling in the chest, often after meals or while lying down.
Common symptoms include:
• Burning sensation in the chest (heartburn)
• Sour or bitter taste in the mouth
• Regurgitation of food or acid
• Discomfort after heavy or late meals
• Symptoms worsening on lying down
Occasional symptoms are usually not serious. However, if these complaints become frequent or troublesome, they may indicate GERD.
Medical Students
GERD is defined as the reflux of gastric contents into the esophagus causing troublesome symptoms or complications.
Key Concepts
• Lower esophageal sphincter (LES) dysfunction is central
• Transient LES relaxation is a major mechanism
• Diagnosis is largely clinical in typical cases
Investigations (When Indicated)
• Upper GI endoscopy
• pH monitoring
• Manometry (in selected cases)
GERD should be differentiated from other causes of chest pain and dyspepsia.
Young Doctors
GERD requires a practical and symptom-oriented approach.
Clinical considerations:
• Typical symptoms often suffice for diagnosis
• Trial of proton pump inhibitors (PPIs) can be both diagnostic and therapeutic
• Always look for alarm features:
• Dysphagia
• Weight loss
• Persistent vomiting
• GI bleeding
Avoid unnecessary investigations in straightforward cases, but do not miss serious pathology.
General Practitioners
GERD is extremely common in primary care.
Practical Approach
• Focused history:
• Relation to meals
• Aggravating factors
• Response to antacids
• Minimal investigations unless red flags are present
Management Principles
• Lifestyle modification:
• Avoid late-night meals
• Reduce fatty and spicy foods
• Elevate head end of bed
• Pharmacological therapy:
• Proton pump inhibitors (e.g., omeprazole)
• H2 blockers (in selected cases)
Patient education plays a major role in long-term control.
Pathophysiology
GERD primarily results from dysfunction of the lower esophageal sphincter (LES).
Key mechanisms include:
• Transient LES relaxation
Allows gastric contents to reflux into the esophagus
• Increased intra-abdominal pressure
Seen in obesity, pregnancy, or tight clothing
• Delayed gastric emptying
Prolongs exposure of acid
• Esophageal mucosal sensitivity
Leads to symptom perception even with minimal reflux
Repeated exposure of the esophageal lining to acid results in irritation, inflammation, and in some cases, structural changes.
When to See the Doctor
Medical evaluation is necessary if:
• Symptoms occur frequently (more than 2–3 times per week)
• There is difficulty in swallowing
• There is unexplained weight loss
• There is vomiting or evidence of bleeding
• Symptoms persist despite medication
Early consultation helps prevent complications.
GERD is a condition of imbalance—where a normally controlled physiological process becomes persistent and harmful. It reflects the failure of a protective mechanism rather than the presence of a structural defect.
For the physician, it requires a balanced approach—recognizing common patterns while remaining alert to warning signs.
For the patient, it emphasizes the importance of lifestyle, timing of meals, and adherence to treatment.
In GERD, control is achievable—not merely through medication, but through understanding and correcting the underlying habits that sustain it.
Dos and Don’ts
Do
• Eat smaller, regular meals
• Avoid lying down immediately after eating
• Maintain a healthy weight
• Elevate the head end during sleep
• Take medications as prescribed
Don’t
• Consume excessive spicy or fatty foods
• Eat late at night
• Smoke or consume alcohol excessively
• Ignore persistent symptoms
• Self-medicate long-term without advice
FAQs About GERD
1. Is GERD the same as acidity?
Not exactly. Occasional acidity is common, but GERD is a persistent condition.
2. Can GERD cause chest pain?
Yes. It can mimic heart-related chest pain.
3. Is GERD a lifelong disease?
It can be controlled effectively with lifestyle changes and medication.
4. Are PPIs safe for long-term use?
Generally safe when used under medical supervision.
5. Can GERD lead to serious complications?
Yes, if untreated, it may lead to esophagitis or other complications.

By Dr. Mohammed Tanweer Khan
A Proactive/Holistic Physician
Founder of WithinTheBody.com